Shoulder arthritis
 Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026
Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026Shoulder arthritis is wear and damage to the smooth cartilage lining the ball-and-socket (glenohumeral) joint, causing deep pain, stiffness, and loss of movement. It can develop as wear-and-tear osteoarthritis, follow a massive rotator cuff tear (cuff tear arthropathy), be part of rheumatoid arthritis, or follow a previous fracture. Treatment ranges from pain relief, physiotherapy, and injections through to shoulder replacement in advanced cases.
📊 Shoulder arthritis is less common than arthritis of the hip or knee, as the shoulder is not a weight-bearing joint. It may follow a massive rotator cuff tear (cuff tear arthropathy), rheumatoid arthritis, a previous fracture, or develop as wear-and-tear osteoarthritis. Where replacement is needed, reverse shoulder replacement is now the most commonly implanted type in the UK.

What is shoulder arthritis?
Arthritis means loss of the smooth cartilage that normally lets the joint surfaces glide over each other. As the cartilage of the ball-and-socket (glenohumeral) joint wears away, the bones begin to rub together, causing deep shoulder pain, stiffness, a grating or clicking sensation (crepitus), and a gradual loss of movement in all directions.
Several forms affect the shoulder. Wear-and-tear osteoarthritis can arise on its own or after a previous injury. Rotator cuff arthropathy is arthritis combined with a massive rotator cuff tear, and the state of the cuff changes which treatments are suitable. Rheumatoid and other inflammatory arthritis cause the joint lining to become inflamed and progressively damage cartilage and bone. Less commonly, arthritis follows loss of blood supply to the humeral head (avascular necrosis).
Symptoms usually build up slowly, and many people manage well for a long time with pain relief, activity changes, physiotherapy, and injections. Surgery is considered once pain and stiffness significantly affect daily life and non-surgical treatment is no longer helping. Where the joint is severely worn, shoulder replacement gives reliable pain relief: recovery takes 6–12 months, and most patients achieve significant pain relief and improved daily function.
Common causes
- Wear-and-tear osteoarthritis of the glenohumeral joint (primary or secondary)
- Rotator cuff arthropathy (arthritis combined with massive rotator cuff tear)
- Rheumatoid arthritis affecting the shoulder joint
- Avascular necrosis of the humeral head
- Previous shoulder fracture or dislocation (post-traumatic arthritis)
- Previous shoulder surgery or joint infection
Who is at risk? Advanced age, inflammatory arthritis, previous shoulder injury or surgery, and heavy occupational or sporting demands are the main risk factors for developing shoulder arthritis.
Symptoms
Symptoms vary depending on the severity and duration of the condition. Common symptoms include:
- Deep aching pain within the shoulder joint, often poorly localised
- Pain at rest and at night, disrupting sleep
- Progressive loss of shoulder movement in all planes
- Crepitus (grinding or clicking) with shoulder movement
- Weakness and reduced function for daily activities
- In rotator cuff arthropathy: significant weakness as well as pain and stiffness
When to seek help: See your GP or a shoulder specialist if shoulder pain is severe, not responding to pain relief and physiotherapy, and significantly affecting quality of life or sleep. Shoulder replacement is considered only when non-operative measures have been exhausted.
How is it diagnosed?
Your surgeon will take a detailed history and examine the joint. The following investigations may be arranged to confirm the diagnosis:
- X-ray - AP, lateral, and axillary views show joint space loss, osteophytes, and humeral head migration
- CT scan - essential for surgical planning, assessing glenoid morphology (Walch classification) and bone stock
- MRI - assesses rotator cuff integrity, which determines the type of replacement
- Bone density assessment in osteoporotic patients
Glenoid morphology on CT directly influences the surgical plan. Posterior glenoid wear and retroversion may require augmented glenoid components or bone grafting. Rotator cuff integrity on MRI is the key determinant of whether to perform anatomical or reverse replacement.
Treatment pathway
Treatment is tailored to the severity of the condition, your age, activity level, and overall health. Most conditions are treated in a stepwise fashion, starting with the least invasive options.
Non-operative management
Analgesia, physiotherapy, activity modification, and intra-articular steroid or hyaluronic acid injections should all be tried before surgery. These rarely cure end-stage arthritis but may control symptoms for a period.
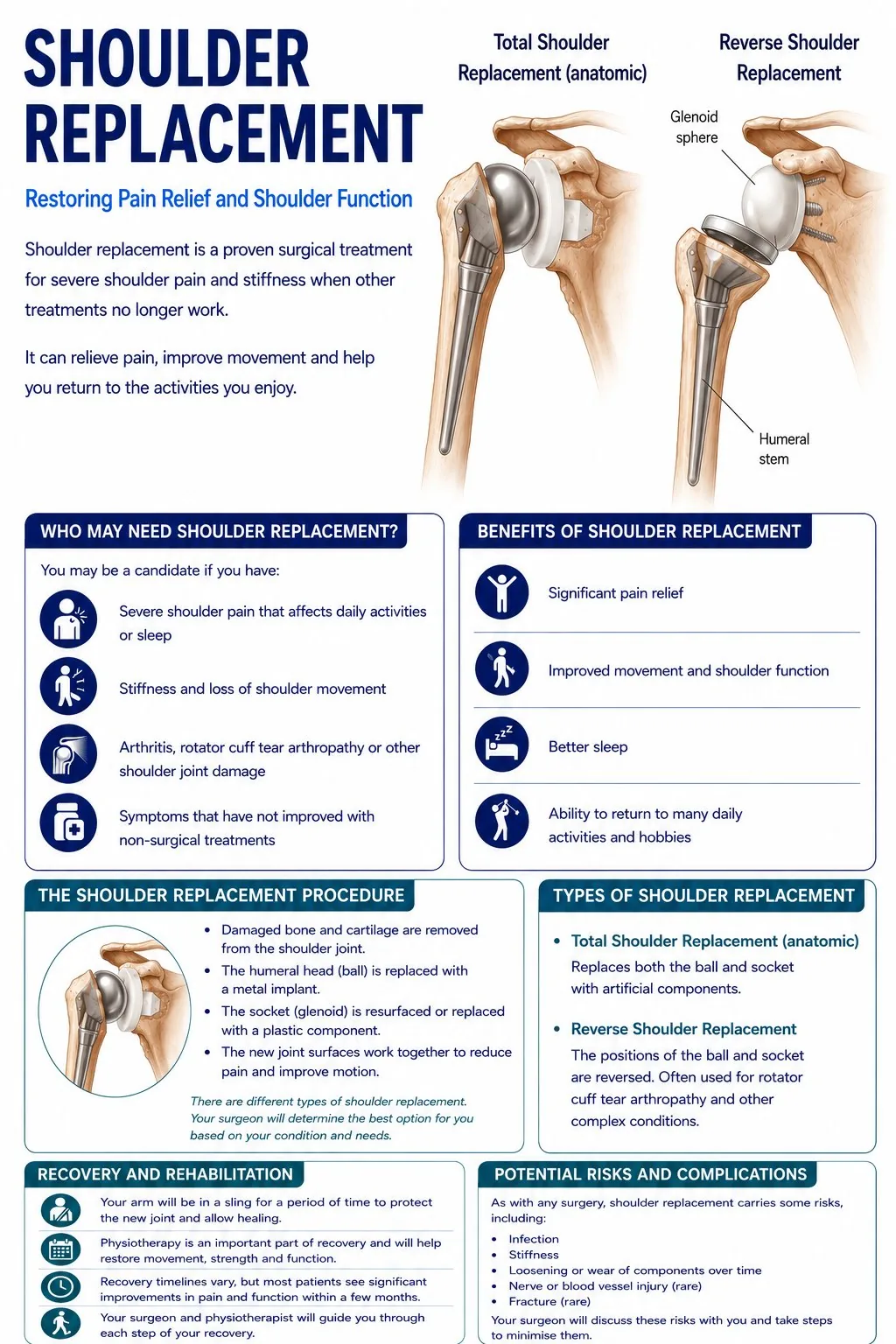
Total anatomical shoulder replacement
Resurfacing of the humeral head and glenoid with a metal humeral component and a polyethylene glenoid component. Predictable pain relief with good restoration of movement in patients with glenohumeral OA and an intact rotator cuff.
Reverse shoulder replacement
The inverted geometry allows the deltoid to compensate for the absent rotator cuff. Highly effective for pain relief; forward flexion usually achieves 120-140 degrees post-operatively. The most commonly performed shoulder arthroplasty in the UK.
Hemiarthroplasty
Replaces the humeral head only, preserving the native glenoid. Used for complex fractures in elderly patients and in selected elective cases such as isolated humeral head avascular necrosis with a well-preserved glenoid, or in younger patients where glenoid preservation is preferred.
Recovery
Many people manage shoulder arthritis for years with pain relief, physiotherapy, activity changes, and injections. If replacement is needed, most patients notice significant pain relief within weeks of surgery, and movement returns over months with physiotherapy; patients with reverse replacement generally recover function faster. Strenuous overhead activity and heavy lifting are generally restricted permanently after replacement.
- Non-surgical treatment: ongoing
- Sling after replacement: 4-6 weeks
- Physiotherapy starts: Week 2-4 after replacement
- Return to light activities: 3-6 months
- Maximum improvement: 12-18 months
What results can I expect?
The outlook depends on the type and severity of arthritis and the treatment chosen. Non-surgical measures control symptoms well for many people. Where shoulder replacement is needed, over 90% of patients report significant pain relief and the 10-year survival rate for modern shoulder prostheses exceeds 90%. Glenoid loosening is the most common long-term complication of total anatomical replacement.
Shoulder arthritis - causes and treatment options
Common activity questions for this condition. Timelines are approximate, always follow the specific guidance given by your surgeon and physiotherapist.
| Activity | Typical timeline | Notes |
|---|---|---|
| Drive | Weeks 8–10 | When sling is off and you can safely control the vehicle. Confirm with your surgeon and insurer. |
| Sleep in bed | Weeks 2–4 | Propped up at 45° initially. Most patients return to a normal sleeping position by 3–4 weeks. |
| Shower | Week 1–2 | Once wound is sealed. No submerging (bath/pool) until wound fully healed (~2 weeks). |
| Return to desk work | Weeks 6–8 | Light computer and writing when arm is comfortable. |
| Return to manual work | Months 6–12 | Heavy labour is generally not recommended after shoulder replacement. Discuss with your surgeon. |
| Swimming | Months 3–4 | Gentle breaststroke. Avoid front crawl initially. |
| Golf | Months 4–6 | Light chipping and putting first. Full golf at 6 months if movement allows. |
| Lift 5kg+ | Month 3+ | Avoid heavy lifting permanently, no repetitive loading over 5kg is generally advised. |
Common concerns during recovery, and whether they are expected.
Your questions, answered
Plain-English answers to the things people most often ask, drawn from real patient questions and grounded in published guidance. Tap a question to open it.
This procedureWhat can I expect afterwards, and how long does it last?
Recovery usually means a sling for several weeks then progressive rehabilitation, with steady gains over about six months and strength improving for a year or more. Most people get good pain relief and useful function, and many return to low-impact activities such as walking, swimming, golf and gardening once healed.
After a reverse replacement in particular, the shoulder will not usually regain completely normal strength or extreme overhead reach, and heavy lifting, contact sport and high-impact activity are generally discouraged to protect the implant.
Implant lifeWill the replacement wear out?
Modern implants last a long time: many are still working well at 10 to 15 years and beyond, and for older patients the replacement often lasts the rest of their life. Younger and very active people should understand that an implant has a finite lifespan and may eventually need revision, which is part of why age and activity are weighed up before surgery.
PreparingHow can I prepare, and what should I ask my surgeon?
A bit of preparation makes the first weeks much easier: get as fit and well as you reasonably can, set your home up so things are within reach of your good arm, sort loose front-opening tops and slip-on shoes, and arrange help for the first week or two if you live alone. If you have diabetes, flag it early, as it affects healing and the response to any steroid used around the operation.
Good questions to take to clinic include: exactly what is being done and why; how long in the sling and what type; when physiotherapy starts; what to expect at six weeks, three months and a year; the pain-relief plan and whether you will have a nerve block; when you can shower, drive, work and return to your sport; and the main risks, including the chance of re-tear.
AnaesthesiaWhat is a nerve block, and what happens when it wears off?
A nerve block numbs the nerves to the shoulder and arm, usually alongside a general anaesthetic, and gives excellent pain relief for roughly the first 10 to 24 hours. The arm often feels heavy and numb during that time, which is expected.
As it wears off, usually the evening or night after surgery, pain can return quite suddenly ("rebound pain"). This is well recognised and not a sign anything is wrong. Start your prescribed pain relief on schedule before the block fully wears off, so you stay ahead of it. A hoarse voice, a drooping eyelid, or a feeling of breathlessness can occur as the block spreads to nearby nerves; these settle as it wears off, but tell your anaesthetist beforehand if you have significant lung disease, asthma or sleep apnoea.
Pain & sleepHow will I sleep, and how long will I be in the sling?
Sleep is one of the hardest parts of early recovery. Many people sleep semi-upright in a recliner or well propped up, supporting the operated arm on pillows, and keep the sling on at night for as long as the surgeon advises. Expect broken sleep for several weeks and try not to measure recovery by it.
Sling time varies with the operation, commonly around the first six weeks for a repair. Neck and upper-back ache from the strap is very common; easing and padding the strap helps, as do gentle hand, wrist and elbow movements. Do not stop the sling early just to get comfortable; wait until your surgeon clears it.
Pain & medsWhat can I take for pain, and what if I cannot tolerate strong painkillers?
Pain is usually managed with a combination: the nerve block, regular paracetamol, an anti-inflammatory if safe for you, a short course of a stronger painkiller for the first few days, and ice. Using several milder approaches together often works better, with fewer side effects, than one strong drug.
If opioids make you sick, or you cannot take anti-inflammatories (stomach, kidney, heart or stroke history), this is common, so tell your team in advance to plan around it. One point that causes confusion: ketorolac (Toradol) is an anti-inflammatory given by mouth, muscle or drip, not an injection into the shoulder joint. Your prescriber decides what is safe for you.
Wound & scarsHow do I look after the wound and scars, and when can I shower?
Showering depends on your dressings and your surgeon's advice, so follow the instruction you were given. Keyhole wounds are small, but the skin around them can feel dry, tight or crispy and catch on clothing; a loose dressing stops it rubbing, and once fully healed a plain moisturiser can settle the dryness.
The incision points can stay tender for several weeks, which is normal. Once healed, gentle scar massage (your physiotherapist can show you) reduces sensitivity over time, and it is worth protecting healing scars from strong sun. Do not put creams on a wound that is not yet closed, and report spreading redness, heat, discharge or fever.
Getting backWhen can I drive and return to work?
There is no single fixed date, and it is ultimately your responsibility to be safe and legal. As a rough guide, UK services often suggest driving around six to eight weeks after a repair, when you can control the car and perform an emergency stop confidently without significant pain, and you are not taking medication that affects alertness. It is also sensible to check your motor insurance position first.
Desk work is often possible around six to eight weeks, and heavier manual work around four to six months, depending on the job and the operation. Your surgeon's specific advice always takes priority.
WellbeingIs it normal to feel low during recovery?
Yes, and it is talked about far too little. Frustration, low mood, isolation and poor sleep are common while you are in a sling and reliant on others, and it does not mean recovery is going badly. Keeping gently active within your limits, staying connected to people, and marking small milestones all help.
If low mood is persistent, deepening, or affecting daily life, please speak to your GP. Effective support is available and asking early is a strength.
Your choiceCan I ask for a second opinion?
Yes. Wanting to understand your diagnosis and feel heard is reasonable, and a second opinion is a normal part of healthcare, not a criticism of anyone. You are entitled to ask your clinician to explain your scan and the reasoning, what the alternatives are, and what happens if you do nothing.
If you are still unsure, another shoulder specialist's view is a legitimate next step. Bring your imaging and a written list of questions, and be specific about your goals and what the shoulder stops you doing.
UrgentWhen should I seek urgent help?
Most shoulder problems are not dangerous, but a few warning signs deserve prompt attention: an unexplained lump that is enlarging, deep or larger than a few centimetres; constant pain at rest and at night that is steadily worsening; feeling generally unwell with weight loss, fevers or night sweats; a sudden inability to lift the arm after an injury; signs of wound infection after surgery (a firm, warm, enlarging or increasingly tender area, spreading redness, discharge or fever); signs of a possible blood clot (new calf pain or swelling, or chest pain or breathlessness); or pain not relieved at all by your prescribed medication.
If you are worried, contact your GP or, after surgery, your surgical team. If you are acutely unwell, use NHS 111 or urgent care.
- Versus Arthritis: Osteoarthritis of the elbow and shoulder
- NICE CKS: Shoulder pain (clinical knowledge summary)
- NHS: Shoulder pain
- British Elbow & Shoulder Society: Patient information
- Cleveland Clinic: reverse shoulder replacement
- Return to sport after shoulder arthroplasty (systematic review)
- ASRA: rebound pain after a nerve block
- StatPearls / OpenAnesthesia: interscalene block side effects
- NHS community MSK service: after rotator cuff repair surgery
- Hospital for Special Surgery: rotator cuff surgery recovery
- NICE NG12 & Cancer Research UK: suspected cancer / soft-tissue sarcoma referral
These links are to UK clinical guidance and patient information from recognised organisations. This page is for general information and does not replace personalised advice from your own clinical team.
Preparing for surgery?
Read our step-by-step guide - what to expect before, during, and after your procedure.
How is it diagnosed?
- ✓X-ray - AP, lateral, and axillary views show joint space loss, osteophytes, and humeral head migration
- ✓CT scan - essential for surgical planning, assessing glenoid morphology (Walch classification) and bone stock
- ✓MRI - assesses rotator cuff integrity, which determines the type of replacement
- ✓Bone density assessment in osteoporotic patients
Recovery milestones
- ●Sling immobilisation: 4-6 weeks
- ●Physiotherapy starts: Week 2-4
- ●Return to light activities: 3-6 months
- ●Maximum improvement: 12-18 months