Frozen shoulder
 Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026
Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026Frozen shoulder (adhesive capsulitis) causes progressive pain and global stiffness of the shoulder joint due to inflammation and contraction of the shoulder capsule. It resolves spontaneously in most patients over 1-3 years.
📊 Frozen shoulder affects approximately 2-5% of the general population and up to 20% of people with diabetes. It is significantly more common in women and in those with thyroid disorders.

What is a frozen shoulder?
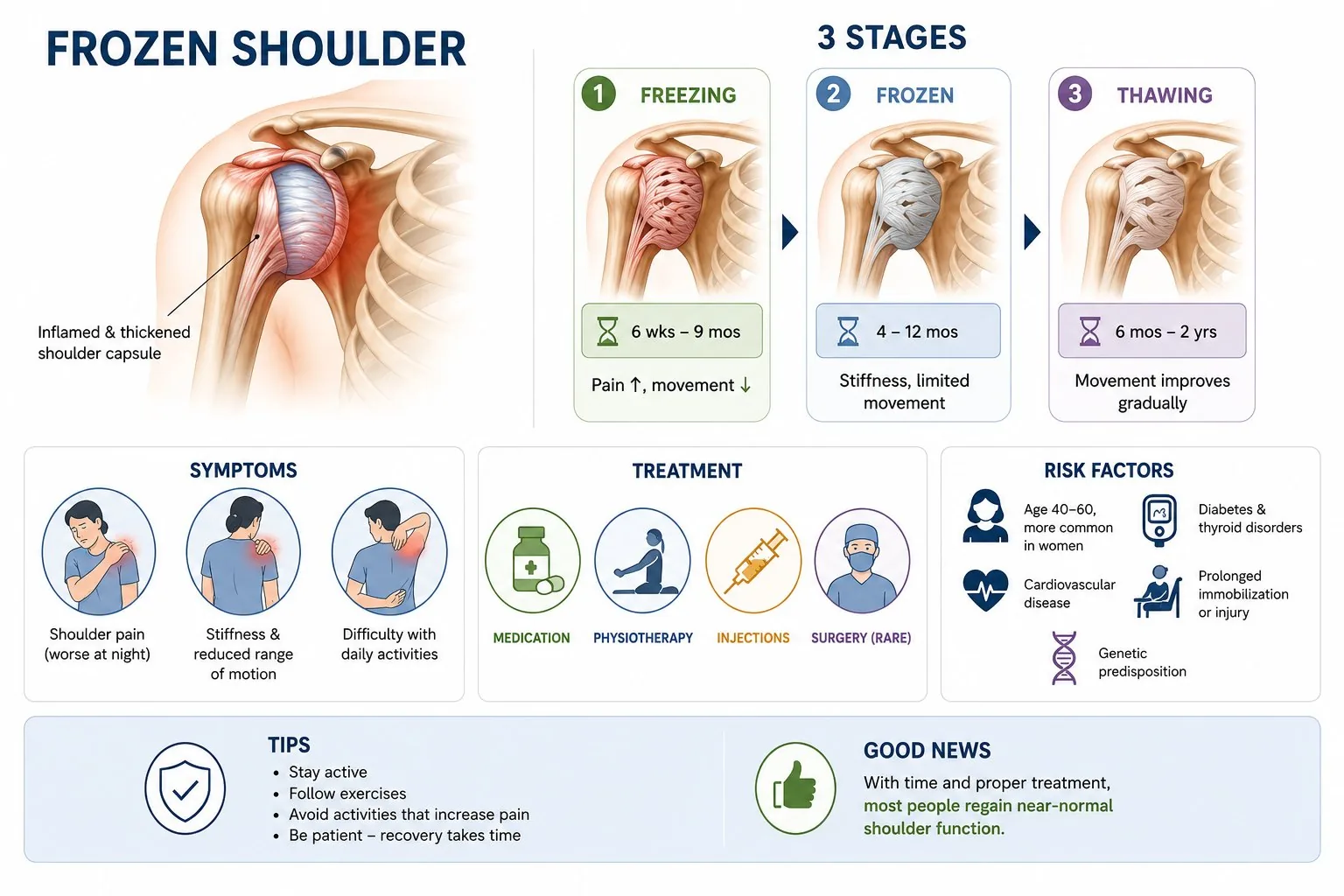
Frozen shoulder, also called adhesive capsulitis, is a condition where the lining of the shoulder joint tightens and shrinks, causing pain and significant loss of movement. It typically goes through three stages: a painful freezing stage (lasting weeks to months), a stiff frozen stage (months to over a year), and a gradual thawing stage where movement slowly returns.
The cause is not fully understood, but frozen shoulder is more common in people with diabetes, thyroid problems, or a history of shoulder injury or surgery. It is most often seen in people aged 40–60, and is more common in women. The condition almost always improves eventually, but this can take one to three years, which can be a difficult thing to hear when you are in pain.
A steroid injection into the shoulder is most effective when given in the early painful stage and can significantly reduce pain and speed recovery. Hydrodilatation (inflating the joint with fluid) and physiotherapy are also used. For patients who do not improve, keyhole surgery to release the tight capsule can give rapid improvement, but requires intensive physiotherapy afterwards to maintain the gains.
Common causes
- Idiopathic (no identifiable cause in most cases)
- Diabetes mellitus - the most important systemic risk factor
- Thyroid disorders (both hypothyroidism and hyperthyroidism)
- Previous shoulder injury or surgery
- Prolonged immobilisation of the arm
- Cardiovascular disease and Dupuytren disease (associated conditions)
Who is at risk? Women aged 40-60 are most commonly affected. Diabetes increases the risk three to five times and is associated with a more resistant, prolonged course. Approximately 10-15% of patients will eventually develop frozen shoulder in the opposite shoulder.
Symptoms
Symptoms vary depending on the severity and duration of the condition. Common symptoms include:
- Severe aching pain at the shoulder, often worse at night and when lying on the affected side
- Progressive loss of all shoulder movements, both active and passive
- Inability to reach behind the back, to the side, or above the head
- Loss of external rotation is usually the earliest and most prominent restriction
- Difficulty with daily tasks such as dressing, fastening clothing, or reaching a back pocket
- In the freezing stage, pain often dominates over stiffness
When to seek help: See your GP if shoulder pain and stiffness has not improved after 4-6 weeks. Early physiotherapy and consideration of steroid injection in the freezing stage may accelerate recovery. Seek assessment for diabetes and thyroid disease if not already investigated.
How is it diagnosed?
Your surgeon will take a detailed history and examine the joint. The following investigations may be arranged to confirm the diagnosis:
- Clinical examination - global restriction of passive movement in all planes, particularly external rotation
- X-ray - usually normal; performed to exclude other causes such as osteoarthritis or calcific tendinitis
- MRI - can confirm capsular thickening and synovitis; useful to exclude a concomitant rotator cuff tear
- Ultrasound-guided injection - can confirm diagnosis and provide treatment simultaneously
The key distinguishing feature from rotator cuff tear is global loss of PASSIVE movement in all planes. Rotator cuff tears predominantly reduce active rather than passive movement. If passive movement is globally restricted, think frozen shoulder rather than rotator cuff.
Treatment pathway
Treatment is tailored to the severity of the condition, your age, activity level, and overall health. Most conditions are treated in a stepwise fashion, starting with the least invasive options.
Corticosteroid injection and physiotherapy
An intra-articular corticosteroid injection provides significant pain relief and can accelerate recovery through the freezing stage. Physiotherapy should accompany injection, focusing on maintaining range of movement and preventing further stiffness.
Home stretching programme
A consistent home stretching programme is essential throughout all stages. Pendulum exercises, passive stretching into external rotation, and behind-the-back stretches are the mainstay. Gentle sustained stretching rather than aggressive forced movement.
Hydrodilatation (distension arthrography)
The shoulder joint capsule is injected with a large volume of fluid (saline and steroid) under imaging guidance to stretch the contracted capsule. Effective in accelerating recovery, particularly in the frozen stage. Performed as an outpatient procedure.
Arthroscopic capsular release
Surgical division of the contracted capsule under general anaesthetic. Reserved for patients who have not responded to 6-12 months of conservative management. Provides rapid resolution of stiffness and requires intensive physiotherapy in the immediate post-operative period.
Recovery
Most patients recover full or near-full shoulder movement with time, but the natural history is prolonged. Injection and physiotherapy can significantly accelerate recovery. Surgical release achieves rapid improvement in movement, followed by intensive rehabilitation. Diabetic patients have a longer and more resistant course.
- Freezing stage: 6 weeks to 9 months
- Frozen stage: 4 to 12 months
- Thawing stage: 6 months to 2 years
- Total natural history: 1 to 3 years
What results can I expect?
The long-term prognosis is generally good - the majority of patients regain near-normal function over 1-3 years. However, up to 40% report some persistent limitation of movement or mild discomfort at long-term follow-up. Diabetic patients have a less favourable prognosis and are more likely to require intervention.
Frozen shoulder - the three stages explained
Common activity questions for this condition. Timelines are approximate, always follow the specific guidance given by your surgeon and physiotherapist.
| Activity | Typical timeline | Notes |
|---|---|---|
| Drive | When safe | When you can perform an emergency stop without pain. May be weeks or months depending on severity. |
| Sleep comfortably | Months 3–18 | Night pain is one of the last symptoms to resolve. A pillow under the arm can help. |
| Shower / hair washing | Immediately | Frozen shoulder does not require surgery for most patients. No wound restrictions. |
| Return to work | Immediately | Desk work usually manageable. Manual work may be limited by pain and stiffness. |
| Swimming | As tolerated | Gentle swimming can help maintain movement. Avoid strokes that cause pain. |
| Golf / sport | As movement allows | Return to sport guided by symptom improvement. Full sport may take 12–24 months. |
| Full shoulder movement | 1–3 years | Most patients regain near-normal movement, but this takes time. Persist with stretching. |
Common concerns during recovery, and whether they are expected.
Your questions, answered
Plain-English answers to the things people most often ask, drawn from real patient questions and grounded in published guidance. Tap a question to open it.
This conditionDoes a frozen shoulder ever actually get better?
Yes. A frozen shoulder is usually self-limiting: it tends to improve and resolve on its own, although this can take a long time. It moves through a painful "freezing" phase, a stiff "frozen" phase, and a gradual "thawing" phase, commonly over one to three years.
Treatment aims to ease pain and speed the return of movement rather than force a cure, and most people regain near-normal function. Recovery can be slower in people with diabetes.
TreatmentWhat treatments work, and is surgery better?
The large UK FROST trial compared early structured physiotherapy with a steroid injection, manipulation under anaesthesia, and arthroscopic capsular release. At twelve months, none was clearly superior for patient-reported pain and function; serious complications were rare but occurred mainly in the surgical groups, and manipulation was the most cost-effective hospital treatment.
In practice, structured physiotherapy with a steroid injection is a reasonable, lower-risk first option, and surgery is not automatically better. Where stiffness is still disabling after several months, manipulation or capsular release may be discussed.
CausesIs it linked to diabetes, thyroid problems or the menopause?
Often there is no obvious trigger, but the strongest associations are with diabetes (where it is more common and more stubborn) and thyroid disorders; roughly 10 to 20 percent of people with diabetes develop a frozen shoulder. It can also follow a period of the shoulder being immobilised, or injury or surgery, and is most common between about 40 and 60 and in women.
There is growing interest in hormonal influences around the menopause, but that remains an area of research rather than settled fact. If there is no clear cause, your GP may check for diabetes or thyroid problems.
InjectionsDo cortisone injections work, and is it bad to have repeated ones?
A steroid injection can give short-term pain relief, particularly in the painful phase of a frozen shoulder. For rotator cuff-related pain the benefit is more modest, tends to last weeks rather than months, and works best alongside an exercise programme.
On repeated injections, caution is reasonable: there is no strong evidence behind the common "rule of three", and steroid around the cuff tendons can, with frequent use, weaken tendon tissue. In diabetes it can also raise blood sugar for a day or two. They are a useful tool used thoughtfully and in limited numbers.
PreparingHow can I prepare, and what should I ask my surgeon?
A bit of preparation makes the first weeks much easier: get as fit and well as you reasonably can, set your home up so things are within reach of your good arm, sort loose front-opening tops and slip-on shoes, and arrange help for the first week or two if you live alone. If you have diabetes, flag it early, as it affects healing and the response to any steroid used around the operation.
Good questions to take to clinic include: exactly what is being done and why; how long in the sling and what type; when physiotherapy starts; what to expect at six weeks, three months and a year; the pain-relief plan and whether you will have a nerve block; when you can shower, drive, work and return to your sport; and the main risks, including the chance of re-tear.
AnaesthesiaWhat is a nerve block, and what happens when it wears off?
A nerve block numbs the nerves to the shoulder and arm, usually alongside a general anaesthetic, and gives excellent pain relief for roughly the first 10 to 24 hours. The arm often feels heavy and numb during that time, which is expected.
As it wears off, usually the evening or night after surgery, pain can return quite suddenly ("rebound pain"). This is well recognised and not a sign anything is wrong. Start your prescribed pain relief on schedule before the block fully wears off, so you stay ahead of it. A hoarse voice, a drooping eyelid, or a feeling of breathlessness can occur as the block spreads to nearby nerves; these settle as it wears off, but tell your anaesthetist beforehand if you have significant lung disease, asthma or sleep apnoea.
Pain & sleepHow will I sleep, and how long will I be in the sling?
Sleep is one of the hardest parts of early recovery. Many people sleep semi-upright in a recliner or well propped up, supporting the operated arm on pillows, and keep the sling on at night for as long as the surgeon advises. Expect broken sleep for several weeks and try not to measure recovery by it.
Sling time varies with the operation, commonly around the first six weeks for a repair. Neck and upper-back ache from the strap is very common; easing and padding the strap helps, as do gentle hand, wrist and elbow movements. Do not stop the sling early just to get comfortable; wait until your surgeon clears it.
Pain & medsWhat can I take for pain, and what if I cannot tolerate strong painkillers?
Pain is usually managed with a combination: the nerve block, regular paracetamol, an anti-inflammatory if safe for you, a short course of a stronger painkiller for the first few days, and ice. Using several milder approaches together often works better, with fewer side effects, than one strong drug.
If opioids make you sick, or you cannot take anti-inflammatories (stomach, kidney, heart or stroke history), this is common, so tell your team in advance to plan around it. One point that causes confusion: ketorolac (Toradol) is an anti-inflammatory given by mouth, muscle or drip, not an injection into the shoulder joint. Your prescriber decides what is safe for you.
Wound & scarsHow do I look after the wound and scars, and when can I shower?
Showering depends on your dressings and your surgeon's advice, so follow the instruction you were given. Keyhole wounds are small, but the skin around them can feel dry, tight or crispy and catch on clothing; a loose dressing stops it rubbing, and once fully healed a plain moisturiser can settle the dryness.
The incision points can stay tender for several weeks, which is normal. Once healed, gentle scar massage (your physiotherapist can show you) reduces sensitivity over time, and it is worth protecting healing scars from strong sun. Do not put creams on a wound that is not yet closed, and report spreading redness, heat, discharge or fever.
Getting backWhen can I drive and return to work?
There is no single fixed date, and it is ultimately your responsibility to be safe and legal. As a rough guide, UK services often suggest driving around six to eight weeks after a repair, when you can control the car and perform an emergency stop confidently without significant pain, and you are not taking medication that affects alertness. It is also sensible to check your motor insurance position first.
Desk work is often possible around six to eight weeks, and heavier manual work around four to six months, depending on the job and the operation. Your surgeon's specific advice always takes priority.
WellbeingIs it normal to feel low during recovery?
Yes, and it is talked about far too little. Frustration, low mood, isolation and poor sleep are common while you are in a sling and reliant on others, and it does not mean recovery is going badly. Keeping gently active within your limits, staying connected to people, and marking small milestones all help.
If low mood is persistent, deepening, or affecting daily life, please speak to your GP. Effective support is available and asking early is a strength.
Your choiceCan I ask for a second opinion?
Yes. Wanting to understand your diagnosis and feel heard is reasonable, and a second opinion is a normal part of healthcare, not a criticism of anyone. You are entitled to ask your clinician to explain your scan and the reasoning, what the alternatives are, and what happens if you do nothing.
If you are still unsure, another shoulder specialist's view is a legitimate next step. Bring your imaging and a written list of questions, and be specific about your goals and what the shoulder stops you doing.
UrgentWhen should I seek urgent help?
Most shoulder problems are not dangerous, but a few warning signs deserve prompt attention: an unexplained lump that is enlarging, deep or larger than a few centimetres; constant pain at rest and at night that is steadily worsening; feeling generally unwell with weight loss, fevers or night sweats; a sudden inability to lift the arm after an injury; signs of wound infection after surgery (a firm, warm, enlarging or increasingly tender area, spreading redness, discharge or fever); signs of a possible blood clot (new calf pain or swelling, or chest pain or breathlessness); or pain not relieved at all by your prescribed medication.
If you are worried, contact your GP or, after surgery, your surgical team. If you are acutely unwell, use NHS 111 or urgent care.
- British Elbow & Shoulder Society: Frozen shoulder
- NICE CKS: Shoulder pain (clinical knowledge summary)
- NHS: Shoulder pain
- British Elbow & Shoulder Society: Early exercises for shoulder problems and sling care
- AAOS OrthoInfo: frozen shoulder
- UK FROST trial (Lancet / NIHR, 2020)
- Corticosteroid injection methods for frozen shoulder: network meta-analysis (Arch Phys Med Rehabil, 2024)
- NIHR Evidence: corticosteroid injections give only short-term relief
- British Elbow & Shoulder Society: patient information
- ASRA: rebound pain after a nerve block
- StatPearls / OpenAnesthesia: interscalene block side effects
- NHS community MSK service: after rotator cuff repair surgery
- Hospital for Special Surgery: rotator cuff surgery recovery
- NICE NG12 & Cancer Research UK: suspected cancer / soft-tissue sarcoma referral
These links are to UK clinical guidance and patient information from recognised organisations. This page is for general information and does not replace personalised advice from your own clinical team.
Preparing for surgery?
Read our step-by-step guide - what to expect before, during, and after your procedure.
How is it diagnosed?
- ✓Clinical examination - global restriction of passive movement in all planes, particularly external rotation
- ✓X-ray - usually normal; performed to exclude other causes such as osteoarthritis or calcific tendinitis
- ✓MRI - can confirm capsular thickening and synovitis; useful to exclude a concomitant rotator cuff tear
- ✓Ultrasound-guided injection - can confirm diagnosis and provide treatment simultaneously
Recovery milestones
- ●Freezing stage: 6 weeks to 9 months
- ●Frozen stage: 4 to 12 months
- ●Thawing stage: 6 months to 2 years
- ●Total natural history: 1 to 3 years