Shoulder instability
 Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026
Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026Shoulder instability describes a spectrum of conditions where the humeral head moves excessively relative to the glenoid, ranging from symptomatic subluxation to frank dislocation. It may be traumatic or atraumatic in origin.
📊 Shoulder dislocation is the most common large joint dislocation. The re-dislocation rate after primary traumatic dislocation exceeds 85% in patients under 20 years of age.

What is shoulder instability?
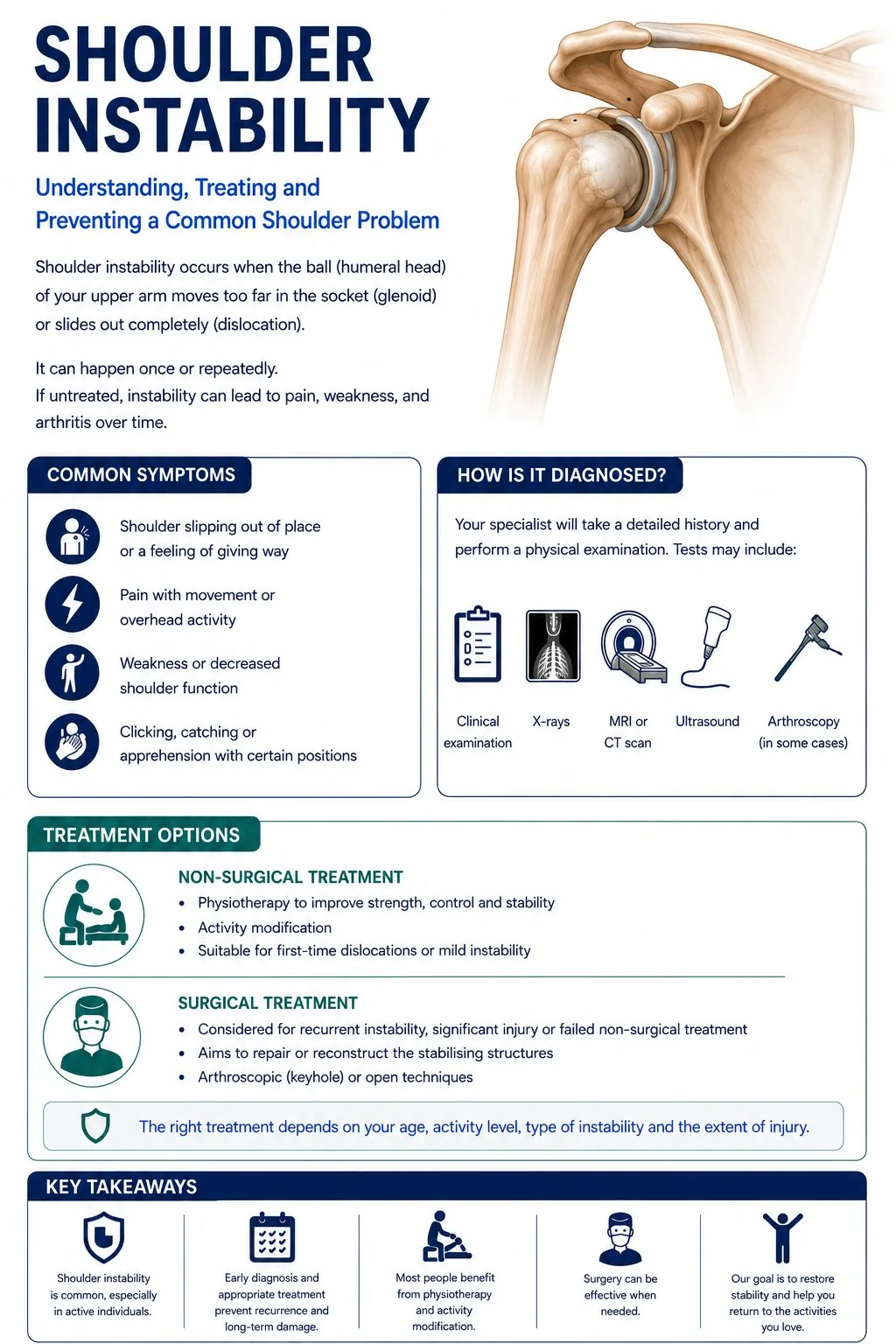
The shoulder is the most mobile joint in the body, it can move in almost any direction. This mobility comes at a price: it is also the joint most likely to dislocate. Shoulder instability means the ball of the shoulder slips partially or fully out of its socket, either after a specific injury (acute dislocation) or repeatedly over time (recurrent instability).
When the shoulder dislocates for the first time, it usually tears a structure called the labrum, a rim of cartilage that deepens the socket and helps keep the ball in place. In younger people, particularly under 25, the risk of the shoulder dislocating again after a first dislocation is very high, over 85% if they return to contact sport. This is why surgery is often recommended in young active patients after a first dislocation.
The choice of operation depends on how much bone has been lost from the socket as a result of repeated dislocations. With minimal bone loss, an arthroscopic (keyhole) repair of the torn labrum (Bankart repair) gives excellent results. When more bone has been lost, a Latarjet procedure, where a small piece of bone is transferred to the front of the socket, provides a more secure repair.
Common causes
- Traumatic anterior dislocation - the most common mechanism
- Bankart lesion (labral detachment) with or without associated Hill-Sachs defect
- Bony Bankart lesion (fracture of the anterior glenoid rim)
- Generalised ligamentous laxity and hypermobility
- Atraumatic multidirectional instability
- Repetitive overhead loading in athletes
Who is at risk? Young age (under 25) is the strongest predictor of recurrence after primary dislocation. Male sex and contact or collision sport participation significantly increase re-dislocation risk. Bony defects increase failure rates of soft tissue repair.
Symptoms
Symptoms vary depending on the severity and duration of the condition. Common symptoms include:
- A sensation of the shoulder slipping, giving way, or dislocating
- Apprehension when the arm up and rotated back
- Acute severe pain and deformity during a complete dislocation
- Recurrent subluxation episodes provoked by specific arm positions
- Dead arm syndrome - transient neurological symptoms in throwers during provocative loading
When to seek help: After a first dislocation, seek assessment within 2-4 weeks. Early MRI identifies associated labral and bony injuries that influence the risk of recurrence and the choice of treatment. Patients with recurrent instability should be referred to a shoulder specialist.
How is it diagnosed?
Your surgeon will take a detailed history and examine the joint. The following investigations may be arranged to confirm the diagnosis:
- Clinical examination - anterior and posterior load and shift, apprehension and relocation tests, sulcus sign for inferior laxity
- X-ray - AP and Velpeau axillary view identify glenoid fractures and Hill-Sachs lesions
- CT scan - essential for quantifying glenoid bone loss (Sugaya classification)
- MRI arthrogram - gold standard for soft tissue labral lesions and rotator cuff integrity
CT quantification of glenoid bone loss is essential before surgery. Loss of over 20-25% of the glenoid is associated with high failure rates of soft tissue Bankart repair alone, favouring the Latarjet procedure in these cases.
Treatment pathway
Treatment is tailored to the severity of the condition, your age, activity level, and overall health. Most conditions are treated in a stepwise fashion, starting with the least invasive options.
Physiotherapy and changing how you use the shoulder
A guided exercise programme to strengthen the rotator cuff and the muscles around the shoulder blade, helping the shoulder stay in place during everyday movements. This works well for instability that has not been caused by an injury, and for first dislocations in older patients (who tend to have lower rates of further dislocations).
Keyhole Bankart repair
Through keyhole incisions, the torn labrum (the rim of cartilage around the socket) and the ligament beneath it are stitched back to the edge of the socket using small anchors. This is a good option when the bone of the socket is intact, and there is not substantial bone loss. Less reliable in young contact athletes with multiple dislocations or where there is significant bone loss.
Latarjet procedure
A small piece of bone is taken from the front of the shoulder blade (the coracoid) and screwed onto the front of the socket. This rebuilds the missing bone and uses the attached tendon to add an extra stabilising sling across the front of the joint. This is usually offered when bone loss is large, after a Bankart repair has failed, or in young contact athletes at high risk of further dislocations.
Bone block (graft) procedures
When bone loss is very large, when a Latarjet has previously failed, or when the surgeon prefers to avoid taking bone from the coracoid, a separate piece of bone graft can be fixed to the front of the socket instead. The graft is usually taken from the pelvic bone (iliac crest) or, less commonly, from a donor (distal tibial allograft). Like the Latarjet, the aim is to rebuild the socket so that the shoulder stays in place.
Chance of further dislocation by age
After a first traumatic shoulder dislocation, the chance of it happening again depends strongly on age and sex - the younger you are, the higher the risk. The figures below are from the British Elbow and Shoulder Society (BESS) and British Orthopaedic Association (BOA) care pathway, and show the estimated chance of another dislocation within 2 years of a first dislocation (based on Robinson et al.).
| Age at first dislocation | Men | Women |
|---|---|---|
| 15 years | 86% | 54% |
| 18 years | 78% | 45% |
| 20 years | 72% | 40% |
| 25 years | 56% | 28% |
| 30 years | 41% | 19% |
| 35 years | 29% | 13% |
These are averages from research data, and an individual person can vary. The steep fall in risk with age is one of the main reasons surgery is more often recommended for younger patients after a first dislocation.
Recovery
Return to contact sport after Bankart repair takes 6 months of structured rehabilitation. The Latarjet procedure has a shorter return-to-sport timeline despite being more extensive, due to the mechanical advantages of bony augmentation.
- Physiotherapy programme: 3-6 months
- After Bankart repair: sling: 3-4 weeks
- Return to contact sport after Bankart: 6 months
- After Latarjet: sling: 4-6 weeks
- Return to contact sport after Latarjet: 4-6 months
What results can I expect?
Arthroscopic Bankart repair gives excellent results in selected patients with recurrence rates of 5-10%. The Latarjet procedure has recurrence rates below 3% and is favoured in high-risk athletes and those with bone loss. Atraumatic instability responds well to physiotherapy in 75-85% of patients.
Shoulder instability - Bankart lesion and surgical options
Common activity questions for this condition. Timelines are approximate, always follow the specific guidance given by your surgeon and physiotherapist.
| Activity | Typical timeline | Notes |
|---|---|---|
| Drive | Weeks 6–8 | When sling is off and you can perform an emergency stop safely. |
| Sleep in bed | Weeks 2–4 | Initially propped up with sling. Most patients sleep comfortably from week 2–4. |
| Return to desk work | Weeks 4–6 | Light office work when comfortable and out of the sling. |
| Gym (lower body) | Weeks 2–4 | Stationary bike and lower body work from early weeks. |
| Non-contact sport | Months 4–5 | Running, cycling, swimming when strength and movement allow. |
| Contact sport (Bankart) | Month 6 | Full contact sport at 6 months after Bankart repair, guided by functional testing. |
| Contact sport (Latarjet) | Months 4–5 | Latarjet allows earlier sport return, typically 4–5 months. |
| Overhead sport | Months 6–9 | Throwing and overhead sport requires full rotator cuff strength, confirm with physio. |
Common concerns during recovery, and whether they are expected.
Your questions, answered
Plain-English answers to the things people most often ask, drawn from real patient questions and grounded in published guidance. Tap a question to open it.
About thisWhat is shoulder instability?
The shoulder is the body’s most mobile joint, which makes it prone to slipping partly (a subluxation) or fully (a dislocation) out of place. This usually follows an injury, but the shoulder can also feel loose from repeated strain or naturally stretchy tissues.
Your choiceDo I need surgery?
After a first traumatic dislocation, many people are treated with physiotherapy. Surgery to repair or tighten the structures is considered when dislocations keep happening, especially in younger, active people who have a higher chance of recurrence. The right path depends on your age, activity and the type of injury.
RecurrenceWill it happen again?
A younger age at the first dislocation strongly raises the chance of further dislocations, and the risk falls with older age. This is a major reason why surgery is discussed with young, active patients. Your surgeon can give you a sense of your individual risk.
Getting backWhat is recovery and return to sport like?
Without surgery: a short period in a sling, then a progressive programme to build strength and control. After surgery: a sling for a few weeks, then staged rehabilitation, with return to contact or overhead sport usually several months later once strength and control have returned.
AnaesthesiaWhat anaesthetic is used for stabilisation surgery?
Stabilisation is usually done under a general anaesthetic, often combined with a nerve block for pain relief afterwards. Your anaesthetist will discuss the options and the temporary arm numbness a block causes.
PreparingHow do I prepare for surgery?
Stabilisation is often keyhole (arthroscopic) day-case surgery. Arrange a sling and help at home, and you will follow a staged rehabilitation plan afterwards.
UrgentWhen should I seek urgent help?
A shoulder that is dislocated and will not go back, numbness or a cold or pale arm, or being unable to move the arm after an injury, all need urgent assessment. Do not try to force the shoulder back yourself.
WellbeingI am anxious it will pop out again.
That is very common and can affect confidence and sleep. A structured rehabilitation programme and clear advice on which positions to be careful with help rebuild trust in the shoulder.
- British Elbow & Shoulder Society: Shoulder instability
- BESS / BOA care pathway: Traumatic anterior shoulder instability (PDF)
- NICE CKS: Shoulder pain (clinical knowledge summary)
- NHS: Shoulder pain
- British Elbow & Shoulder Society: Early exercises for shoulder problems and sling care
These links are to UK clinical guidance and patient information from recognised organisations. This page is for general information and does not replace personalised advice from your own clinical team.
Preparing for surgery?
Read our step-by-step guide - what to expect before, during, and after your procedure.
How is it diagnosed?
- ✓Clinical examination - anterior and posterior load and shift, apprehension and relocation tests, sulcus sign for inferior laxity
- ✓X-ray - AP and Velpeau axillary view identify glenoid fractures and Hill-Sachs lesions
- ✓CT scan - essential for quantifying glenoid bone loss (Sugaya classification)
- ✓MRI arthrogram - gold standard for soft tissue labral lesions and rotator cuff integrity
Recovery milestones
- ●Physiotherapy programme: 3-6 months
- ●After Bankart repair: sling: 3-4 weeks
- ●Return to contact sport after Bankart: 6 months
- ●After Latarjet: sling: 4-6 weeks
- ●Return to contact sport after Latarjet: 4-6 months