Clavicle fracture
 Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026
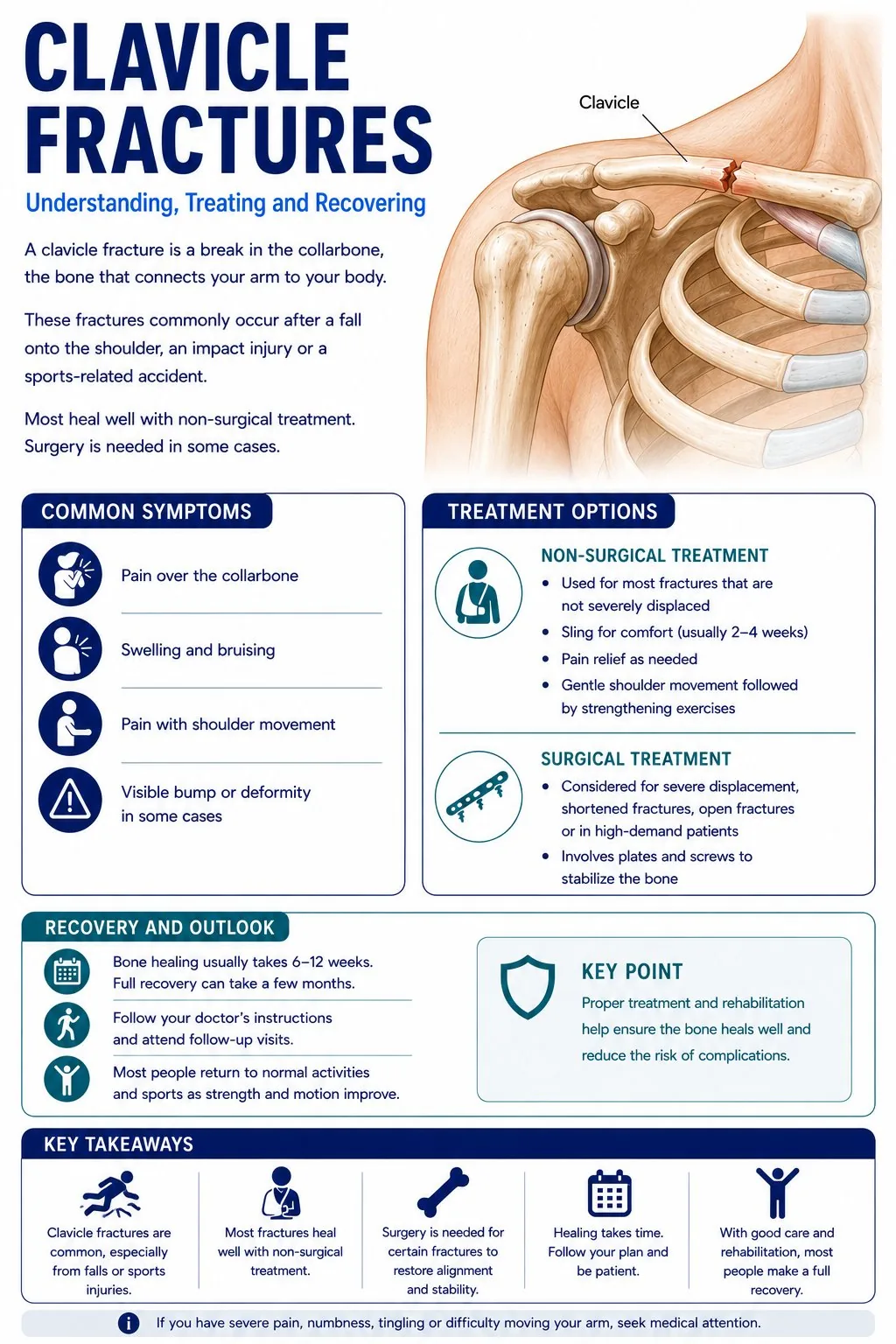
Content reviewed by✓Mr Andrew Davies, PhD FRCS (Tr & Orth) and Mr Andrew Sankey, MA (Cantab) FRCS (Tr & Orth)· Reviewed July 2026A break of the collarbone. This is one of the most commonly broken bones in the body. Most heal well in a sling without surgery, although some patterns of break do better with an operation.
📊 Breaks of the collarbone are very common, especially in children and in active young adults. They make up around 1 in every 25 broken bones seen in hospital. Cyclists, rugby and football players, and people who have fallen from a height are the most common patients.

What is a clavicle fracture?
The collarbone connects the chest to the shoulder. You can feel it as the long horizontal bone running from the front of your throat out to the point of your shoulder. Most breaks happen in the middle of the bone, after a fall onto the shoulder or an outstretched hand.
Most middle-of-the-bone breaks heal well in a simple sling. A firm lump forms at the fracture site over a few weeks as the bone heals, and this is normal. Pain usually settles over the first few weeks. Many people are surprised by how much movement they have even with the bone still healing.
Surgery is sometimes recommended when the broken ends are far apart, when the bone is much shorter than it was before (around 2 cm or more), or when the skin is being pushed up from underneath by a sharp bone fragment. Surgery uses a small plate and screws to hold the bone in the right position while it heals.
Common causes
- A fall onto an outstretched hand or directly onto the shoulder (the most common cause)
- A direct blow to the collarbone
- Cycling crashes, especially going over the handlebars
- Contact sports such as rugby, hockey, and skiing
- Childbirth (a rare cause in newborn babies)
Who is at risk? Young active men, especially aged 15 to 40, are most at risk because of contact sports and cycling. Older people with thinning bones are also at risk after a fall. Newborn babies can occasionally fracture the collarbone during birth, which heals very quickly without treatment.
Symptoms
Symptoms vary depending on the severity and duration of the condition. Common symptoms include:
- Immediate pain at the collarbone after the injury
- A visible lump, bump, or step under the skin over the collarbone
- Swelling and bruising spreading along the top of the shoulder and chest
- Inability to lift the arm without pain
- A grinding feeling or sound at the break when the shoulder is moved
- In rare cases, the skin over the break is tented up by a sharp bone fragment (this needs urgent attention)
When to seek help: Go to A&E soon after a fall with shoulder or collarbone pain. Get seen urgently if you have difficulty breathing, if the skin over the break is dimpled or threatened, or if your fingers feel numb or look pale.
How is it diagnosed?
Your surgeon will take a detailed history and examine the joint. The following investigations may be arranged to confirm the diagnosis:
- Examination of the collarbone, the skin over the break, and the breathing
- X-ray of the collarbone, often with both sides on the same film for comparison
- Checking the pulse at the wrist and the feeling in the hand to make sure no blood vessels or nerves are damaged
- A CT scan in rare cases where the break is in a tricky place (close to the chest or out at the shoulder) or where surgery is being planned
Two things matter most on the X-ray: how much the broken ends have moved apart, and whether the bone is much shorter than it was. Breaks where the bone is shortened by more than around 2 cm are more likely to be offered surgery.
Treatment pathway
Treatment is tailored to the severity of the condition, your age, activity level, and overall health. Most conditions are treated in a stepwise fashion, starting with the least invasive options.
Broad arm sling
A sling is worn for comfort, usually for 2 to 6 weeks. The collarbone heals on its own as you go about daily activities. Gentle pendulum exercises (swinging the arm in small circles) start in the first couple of weeks. A firm lump at the break is normal and shows that bone is forming.
Surgery to fix the bone with a plate
Surgery is offered for breaks where the ends are far apart, where the bone is much shorter than it was, or where the patient is highly active and wants to return to sport as quickly as possible. A small metal plate and screws are placed along the top or front of the bone. Some patients need a second small operation later to take the plate out.
Sling, with careful follow-up
Breaks at the very outer end of the collarbone, close to the shoulder, are watched closely on follow-up X-rays. Some heal well in a sling, but others move with time and may need surgery later.
Recovery
Most collarbone breaks heal without surgery in around 6 to 12 weeks. A firm lump at the break site (the new bone forming) develops and is usually permanent, though it slowly remodels and becomes less noticeable over the first year. Shoulder movement returns quickly once the bone is solid.
- Sling: 2-6 weeks
- Physiotherapy starts: Week 2-4
- Bone heals on X-ray: 6-12 weeks
- Return to non-contact sport: 6-12 weeks
- Return to contact sport: 3-6 months
What results can I expect?
The vast majority of collarbone breaks heal without problems. A small number (around 1 to 5 in every 100) do not heal properly and may need surgery later. People who have surgery as the first treatment usually heal a little faster and have a more normal-looking shoulder, but face the risks of any operation.
Collarbone fracture - when is surgery needed?
Common activity questions for this condition. Timelines are approximate, always follow the specific guidance given by your surgeon and physiotherapist.
| Activity | Typical timeline | Notes |
|---|---|---|
| Drive | Weeks 4–6 | When you can control the vehicle and perform an emergency stop safely. Confirm with insurer. |
| Sleep in bed | Week 1–2 | Most patients manage lying down relatively quickly. Sleeping on the affected side takes longer. |
| Shower | Week 1 | Gentle shower with waterproof dressing. Avoid soaking until wound healed (if surgery). |
| Return to desk work | Weeks 2–3 | One-handed typing initially. Full desk use as arm becomes more comfortable. |
| Cycling | After union confirmed | Road cycling should wait until X-ray confirms union, a further fall risks re-fracture. |
| Contact sport | Weeks 6–12 | Only after X-ray confirms bony union. Do not return based on how it feels. |
| Rugby / horse riding / skiing | Weeks 8–12 | X-ray confirmation of union is mandatory before any contact or high-impact sport. |
Common concerns during recovery, and whether they are expected.
Your questions, answered
Plain-English answers to the things people most often ask, drawn from real patient questions and grounded in published guidance. Tap a question to open it.
About thisWhat is a broken collarbone?
A clavicle (collarbone) fracture is a break in the bone running from the breastbone to the shoulder, usually after a fall onto the shoulder or outstretched arm. Most breaks are in the middle third of the bone.
Your choiceDo I need surgery?
Most collarbone fractures heal well without surgery, supported in a sling. Surgery, using a plate or pin, is considered for badly displaced or shortened breaks, breaks threatening the skin, or certain high-demand situations. Your surgeon weighs healing, function and your activities together with you.
Getting backHow long does it take to heal?
Bone healing usually takes around 6 to 12 weeks, with movement and strength returning over the following weeks to a few months. Return to contact sport is generally later, once the bone has healed and strength is back.
Pain & sleepHow do I manage pain and sleeping?
A sling, simple pain relief and sleeping propped up help in the early weeks. Keep the elbow, wrist and hand moving from the start to prevent stiffness; shoulder movement is introduced as your team advises.
The lumpWill there be a lump where it healed?
A lump of new healing bone is common as the fracture knits, and it often becomes less noticeable over time. Occasionally a break is slow to heal or does not unite, which may need review, so keep your fracture-clinic appointments.
UrgentWhen should I seek urgent help?
Seek urgent review if the skin over the bone looks about to break, if the hand becomes cold, pale or numb, if you are very short of breath, or if a surgical wound becomes hot, red or starts discharging.
WellbeingIt is frustrating being in a sling, is that normal?
Very normal. Early hand and elbow exercises, a clear timeline, and knowing the bone is healing all help. Contact your team if pain or progress is worrying you.
- NHS: Broken collarbone
- British Elbow & Shoulder Society: Early exercises for shoulder problems and sling care
- British Elbow & Shoulder Society: Patient information
These links are to UK clinical guidance and patient information from recognised organisations. This page is for general information and does not replace personalised advice from your own clinical team.
Preparing for surgery?
Read our step-by-step guide - what to expect before, during, and after your procedure.
How is it diagnosed?
- ✓Examination of the collarbone, the skin over the break, and the breathing
- ✓X-ray of the collarbone, often with both sides on the same film for comparison
- ✓Checking the pulse at the wrist and the feeling in the hand to make sure no blood vessels or nerves are damaged
- ✓A CT scan in rare cases where the break is in a tricky place (close to the chest or out at the shoulder) or where surgery is being planned
Recovery milestones
- ●Sling: 2-6 weeks
- ●Physiotherapy starts: Week 2-4
- ●Bone heals on X-ray: 6-12 weeks
- ●Return to non-contact sport: 6-12 weeks
- ●Return to contact sport: 3-6 months